

Ascension Surgical Preference Cards
Enhancing surgical growth and caregiver dignity through the Ascension Surgical Preference Card Editor. A data-backed initiative to reduce surgical friction, improve case readiness, and elevate the caregiver experience across the Ascension network.
Roles
As part of the Experience team, I led the research and service design in collaboration with clinician leadership, facility technology administrators, and contract technology vendors.
I developed a report on the state of digital tools for disease management, captured existing clinical pathways, and translated the research into a prototype service blueprint.
Timeline
The whole team iterated over 3 months.
The project timeline ran from March through May of 2020.
-
We wanted to better understand how healthcare providers and patients could interact with remote monitoring tools to expand workforce capacity and enhance safety during a healthcare surge.
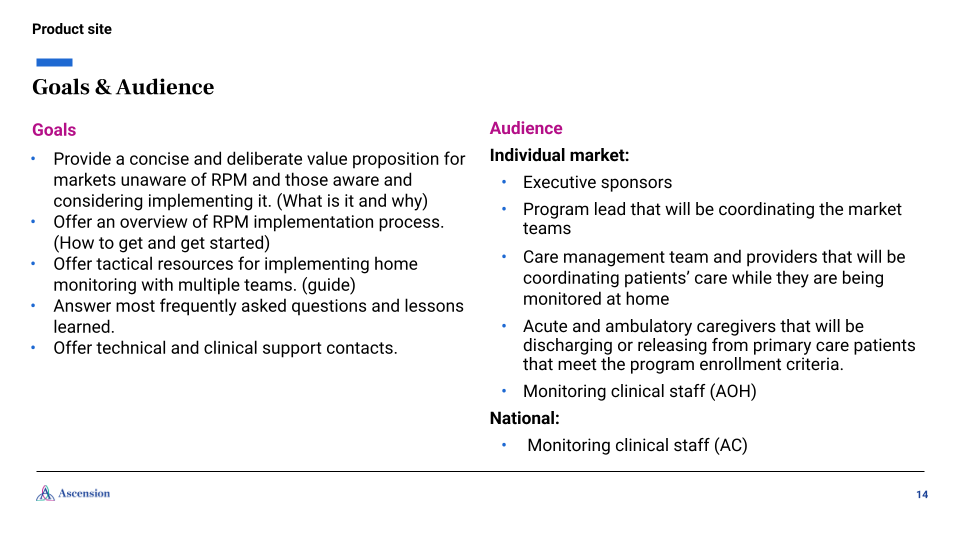
Goals:
Discover emerging practices and tools.
Learn about existing patient remote monitoring for chronic disease, and the frustrations providers face when systems notify them of all data rather than only the most relevant medical data.
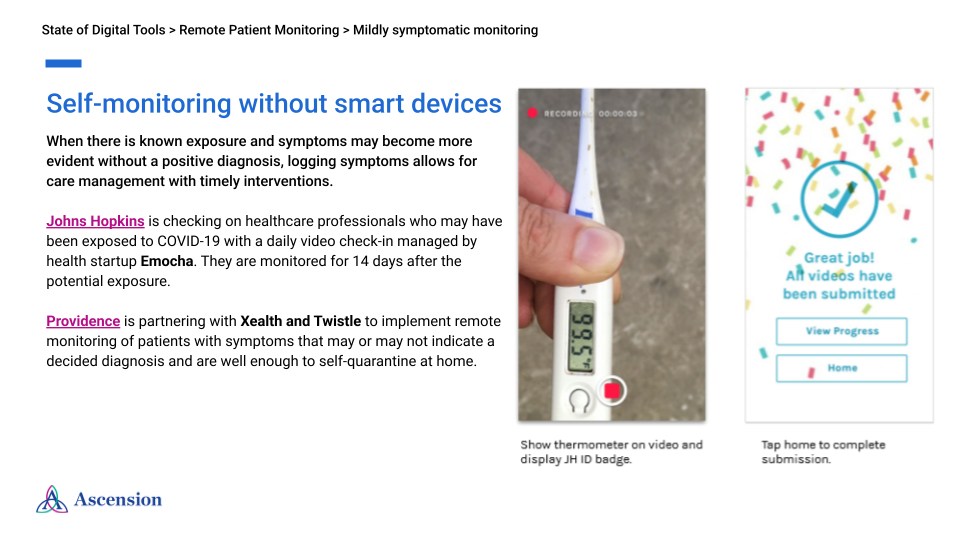
Evaluate how different digital tools could be integrated into existing operations and the four diagnosis stages: Asymptomatic, Mildly Symptomatic, Worsened Symptoms, and Clinician Monitoring.
Visualize & communicate the operational ecosystem for COVID-19 remote patient monitoring.
-
The area of focus was understanding ER rapid-response for patients with worsening symptoms, through the following lines of inquiry:
“Who monitors the patient on a daily basis?”
“What are the clinical protocols for patient monitoring?”
“How do we differentiate between a patient who can self-quarantine and one who requires an ED escalation?”
-
Case Study Reviews: Analyzing how other institutions (e.g., Johns Hopkins, UCSF, Sheba Medical Center) utilized specific hardware and AI to track vitals and predict disease progression.
Stakeholder Inquiries: Gathering pressing questions and daily check-ins from regional implementation teams to prioritize information on the AHM program.
Service Blueprint: Synthesizing findings into a service blueprint that visualized the relationship between patient experience, clinician teams, diagnosis stage, facility capacity, monitoring workflow, and facility administration.
-
Due to the COVID-19 pandemic-related risk factors, we conducted in-depth, remote generative interviews exclusively with clinicians and operations administrators.
Providers: ED/Ambulatory physicians who would discharge patients into the program.
Monitoring Staff: Clinical staff at Ascension Connect (AC) and Ascension On-Hand (AOH) responsible for daily patient management.
Clinical Leadership: VP of Clinical Operations, Regional Technology Officers, and a multitude of administrators involved in emergent services delivery.

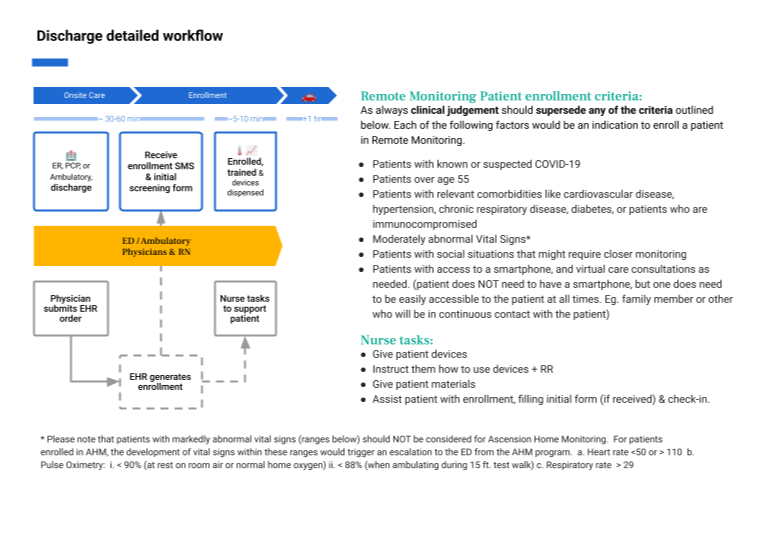
Workflow Diagrams
Mapping the Discharge, Monitoring, and Unenrollment paths to ensure no gaps in care.
Analysis & Synthesis Process
Aggregating clinical pathways for patient management, existing workflows of remote patient monitoring, and individual conversations with facility administrators and technology administrators to understand service gaps.
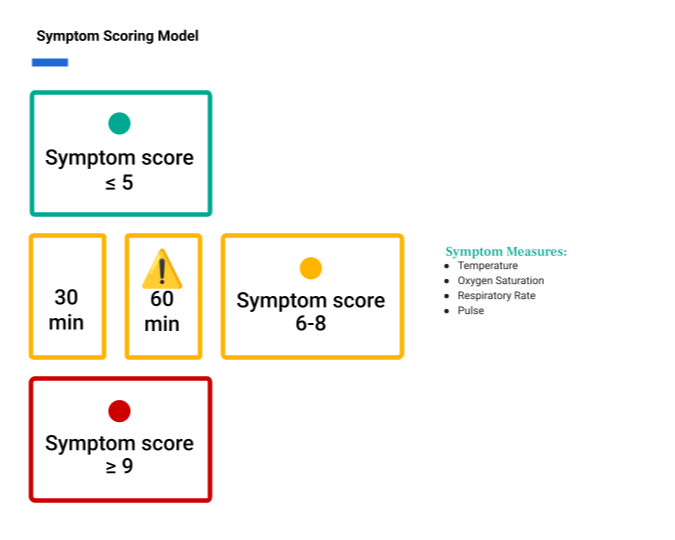
Symptom Scoring Model Mapping
Visualizing a system where symptom scores (e.g., scores of 6-8 vs. ≥9) trigger specific clinical interventions.
Outputs & Deliverables
Patient Service Blueprint: A high-level view of the entire experience
Implementation Playbook: Includes guides for Providers, Nurses, Care Management, and EMS.
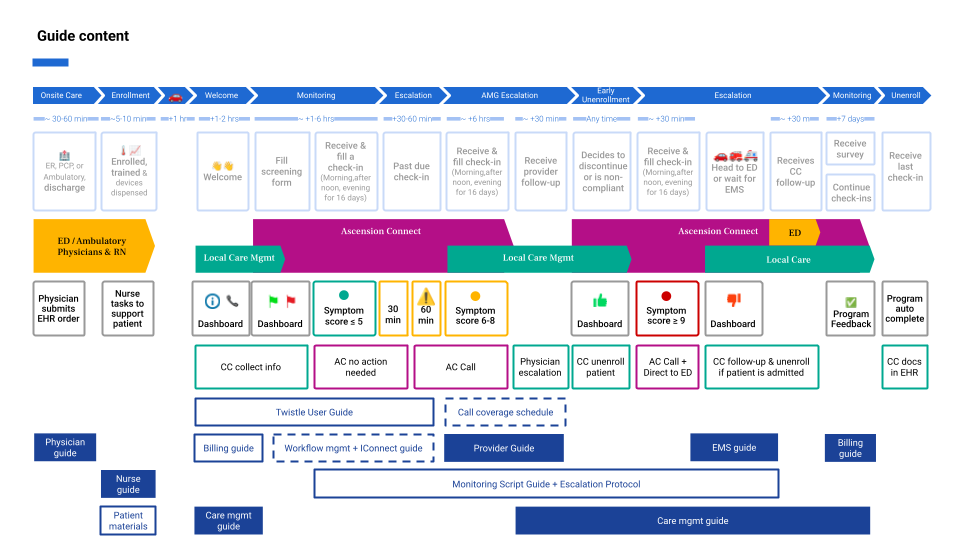
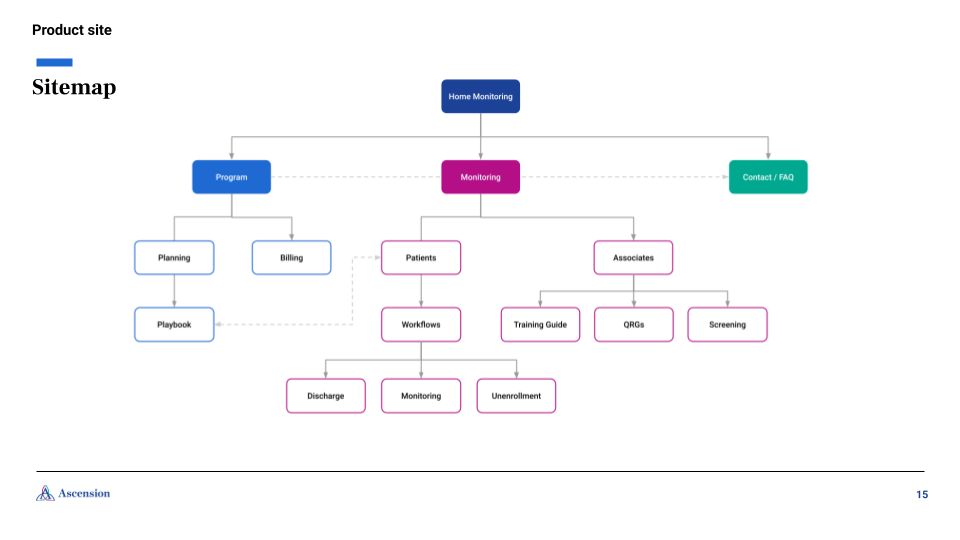
Remote Monitoring Product Site: A centralized hub for clinical leadership and staff to access response protocols, FAQs, and training guides.
Billing Workflow: Detailed guide for using specific codes (99453, 99457, 99458) to ensure the program's financial sustainability.
Impact
The RPM program allowed Ascension to reserve hospital resources for the most critical cases by enabling patients to safely self-report vitals (temperature, O2 saturation, heart rate) from home. It streamlined the escalation protocol, ensuring that only medically relevant data triggered provider alerts, thereby reducing "alert fatigue" and improving provider safety.